Sacroiliac Joint Complex
The sacroiliac joint (SIJ) complex is widely being recognized as major source of chronic lower back pain. In SIJ complex pain, patients tend to complain of buttock pain, but can experience leg pain of involved side as well. Many times this is confused with radicular pain(sciatica) or facet joints pain.
The SIJ complex consists of an articular region, a posterior ligamentous region, a posterior ligamentous region which supports the joints. Neural (nerve) innervations are found in both the posterior capsule of the joint and in tthe posterior sacroiliac and interosseous ligaments. Till now many doctors have used intra-articular (inside joints) injections to both provide relief and to confirm SIJ omplex as source of low backache.
Why endoscopic sacral neurotomy better than conventional RF or Injections
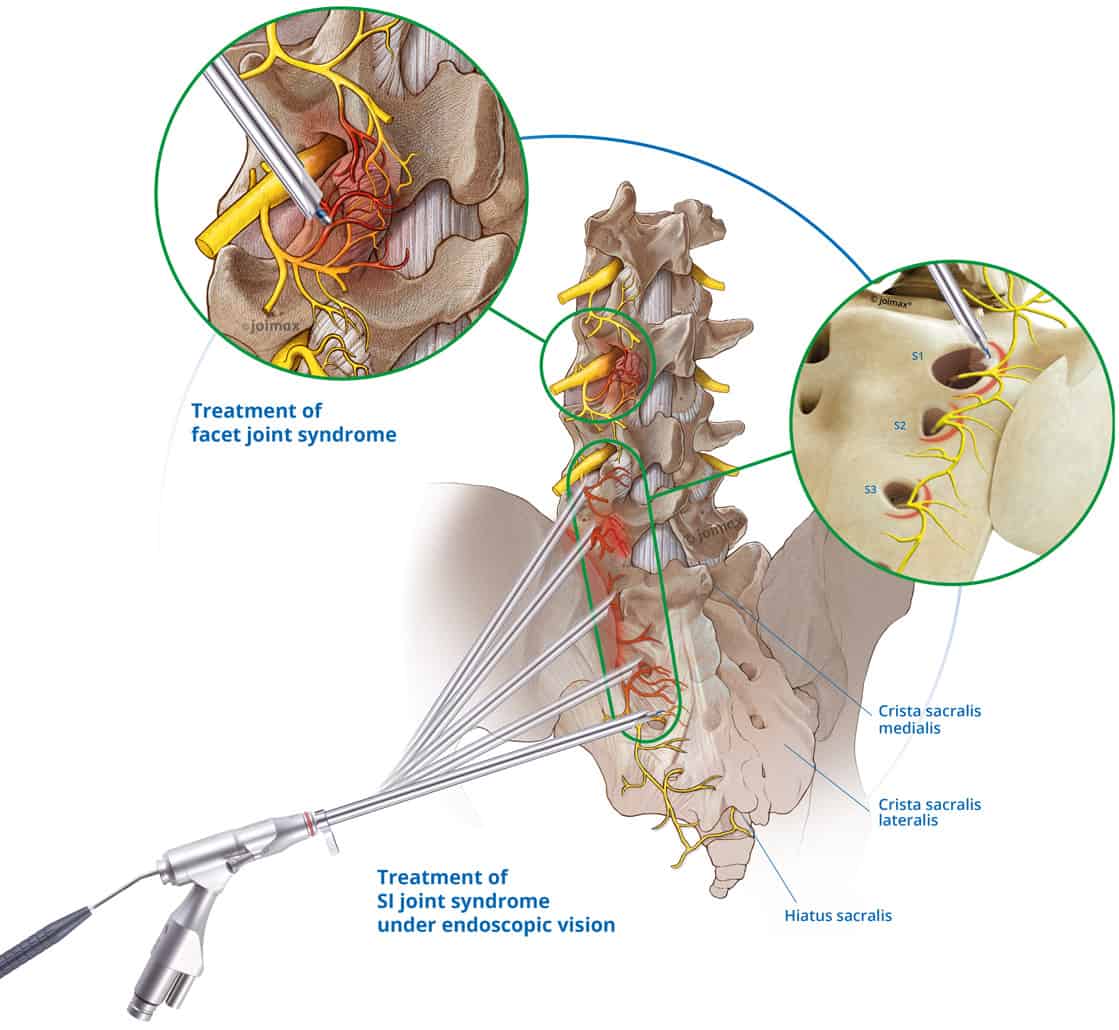
Image courtesy-Joimax
Results from scientific studies have demonstrated, peri-articular structures contributes more to SIJ complex pain than articular region.This suggests peri-articular ligamentous structures as better targets for SIJ pain treatment. This has been proven beyond doubt in a study by drefuss et al that multisite, multidepth lateral sacral branch blocks are more reliable than intra-articular injections for SIJ complex pain relief.
The SIJ complex is innervated by L5-S4 nerves of that side and its locations are quite variable in individual. Current treatment modality such as radiofrequency neurotomy of nerve at periforaminal region are less effective as compared to endoscopic sacral neurotomy.
Advantages
In Endoscopic neurotomy nerves are ablated under direct vision ,thus gives better outcome. In Radiofrequency ablation multiple lesions created, under indirect view.
Another advantage of direct visualization with the endoscope is that it affords us the ability to identify areas that have already been treated/ablated. This allows us to avoid damaging the soft tissue with excessive lesioning of the same region. Avoiding repeated lesioning helps in curbing complications such as post procedural pain and dysthesia. We can say with surety that Endoscopic Sacral Neurotomy is most effective way of treating chronic low back pain associated with sacroiliac joint complex.
Refrences:
- Won-Suh Choi, Jin-Sung Kim, Kyeong-Sik Ryu, Jung-Woo Hur, Ji-Hoon Seong, and Hyun-Jin Cho, “Endoscopic Radiofrequency Ablation of the Sacroiliac Joint Complex in the Treatment of Chronic Low Back Pain: A Preliminary Study of Feasibility and Efficacy of a Novel Technique,” BioMed Research International, vol. 2016, Article ID 2834259, 8 pages, 2016. https://doi.org/10.1155/2016/2834259.
- M. V. Boswell, A. M. Trescot, S. Datta et al., “Interventional techniques: evidence-based practice guidelines in the management of chronic spinal pain,” Pain Physician, vol. 10, no. 1, pp. 7–111, 2007.
- F. D’Orazio, L. M. Gregori, and M. Gallucci, “Spine epidural and sacroiliac joints injections—when and how to perform,” European Journal of Radiology, vol. 84, no. 5, pp. 777–782, 2015.
- R. C. Cox and J. D. Fortin, “The anatomy of the lateral branches of the sacral dorsal rami: implications for radiofrequency ablation,” Pain Physician, vol. 17, no. 5, pp. 459–464, 2014.
- S. M. Aydin, C. G. Gharibo, M. Mehnert, and T. P. Stitik, “The role of radiofrequency ablation for sacroiliac joint pain: a meta-analysis,” PM & R, vol. 2, no. 9, pp. 842–851, 2010.
- Z.-Z. Li, S.-X. Hou, W.-L. Shang, K.-R. Song, and W.-W. Wu, “Evaluation of endoscopic dorsal ramus rhizotomy in managing facetogenic chronic low back pain,” Clinical Neurology and Neurosurgery, vol. 126, pp. 11–17, 2014.
- E. Murakami, Y. Tanaka, T. Aizawa, M. Ishizuka, and S. Kokubun, “Effect of periarticular and intraarticular lidocaine injections for sacroiliac joint pain: prospective comparative study,” Journal of Orthopaedic Science, vol. 12, no. 3, pp. 274–280, 2007.